Prostatic Artery Embolization
Prostatic Artery Embolization (PAE)
Benign Prostatic Hyperplasia (BPH) is a non‑cancerous enlargement of the prostate gland that can narrow the urinary passage and cause bothersome urinary symptoms in men, especially as they grow older.
When medications no longer give adequate relief or cause side‑effects, and you wish to avoid or are not fit for major surgery, Prostatic Artery Embolization offers a minimally invasive, image‑guided treatment option to help improve urinary flow and quality of life.
Minimally Invasive Treatment for Enlarged Prostate
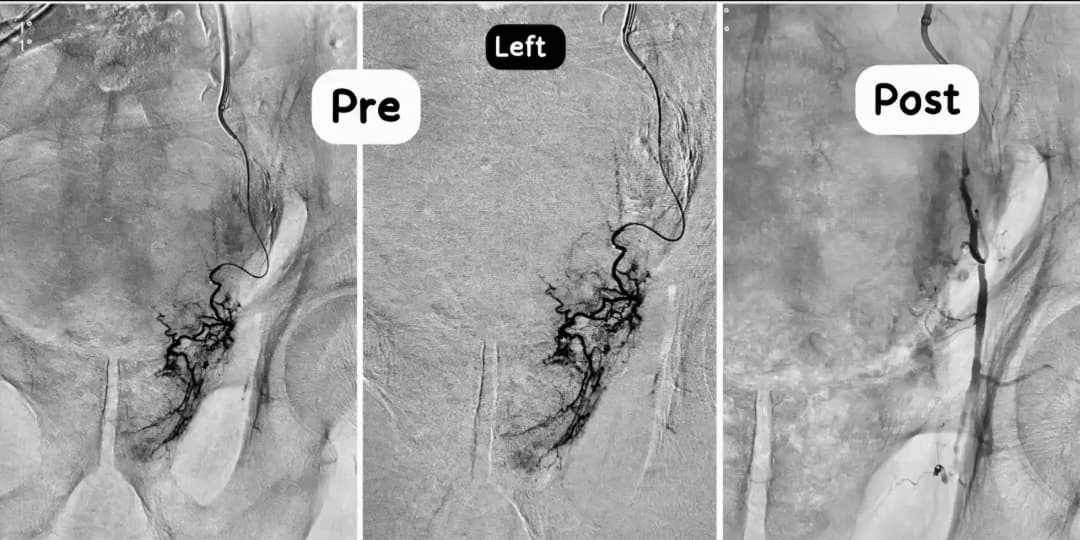
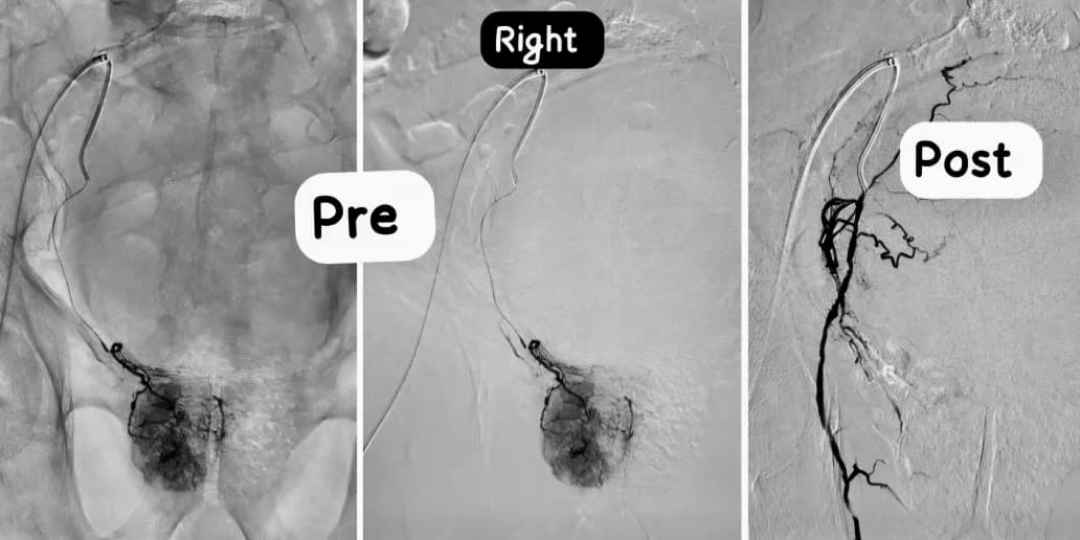
Prostatic Artery Embolization is performed through a tiny puncture in the groin or wrist. Using X‑ray guidance, a thin catheter is navigated into the arteries supplying the prostate, and microscopic particles are injected to reduce its blood supply, causing the gland to gradually shrink.
By reducing the size and congestion of the prostate, PAE can relieve urinary obstruction and associated symptoms in well‑selected patients, often without the need for general anesthesia or a long hospital stay.
Symptoms
BPH‑related prostate enlargement can cause lower urinary tract symptoms such as:
- Frequent urge to pass urine, especially at night (nocturia)
- Weak urinary stream or straining to begin urination
- Feeling of incomplete emptying of the bladder
- Intermittent flow or stopping and starting of urine
- Urgency or leakage if you cannot reach the toilet in time
- Recurrent urinary infections or urinary retention in advanced cases
Treatment
After detailed evaluation, including ultrasound and/or MRI of the prostate and uroflowmetry when required, we discuss whether PAE is suitable. For appropriate candidates, the treatment usually involves:
- Catheterisation of prostatic arteries through a tiny skin puncture under local anesthesia and conscious sedation.
- Targeted embolization with calibrated particles to reduce blood flow to the enlarged prostate while preserving surrounding structures.
- Post‑procedure care with observation, hydration and pain control before going home.
After Treatment
Recovery after PAE is generally smooth, with most patients returning to routine activities soon. We usually advise:
- Plenty of oral fluids and light activity from the same or next day, as advised
- Avoiding heavy lifting or strenuous exercise for a short period
- Regular follow‑up visits with symptom scoring and urine flow assessment
- Reporting any burning while passing urine, fever or severe pelvic pain
Frequently Asked Questions
-
1.Who is a candidate for Prostatic Artery Embolization?
PAE may be considered for men with symptomatic BPH who have moderate to severe urinary symptoms, inadequate relief or side‑effects with medications, or are poor candidates for surgery. Final suitability is decided after clinical assessment, imaging and discussion of all options.
-
2.Is the procedure painful?
PAE is usually done under local anesthesia with light sedation. You may feel some discomfort in the groin or pelvic region during or after the procedure, but this is generally mild and controlled with medicines.
-
3.Will I need hospital admission?
Many patients can go home the same day or after an overnight observation, depending on their general health and response. Your doctor will explain the expected duration of stay before the procedure.
-
4.When will I feel improvement?
Some patients notice improvement in urinary flow and reduction in frequency within weeks, while for others the benefits develop gradually over a few months as the prostate shrinks. Regular follow‑up helps track your response.
-
5.What are the risks?
As with any vascular procedure, there are risks such as bruising at the puncture site, transient urinary burning, infection, allergic reaction to contrast and, rarely, unintended embolization to nearby tissues. We use detailed imaging and meticulous technique to minimise these risks.
-
6.Does PAE replace surgical treatment like TURP?
PAE is an alternative, minimally invasive option for selected men, especially those who are high‑risk for surgery or prefer a catheter‑based approach. In some cases, standard surgical procedures like TURP or other techniques may still be recommended as the best option; your care team will discuss what is most suitable for you.